Brain scans of 3-year old children: normal vs neglected
Excerpt:
Both of these images are brain scans of a two three-year-old children, but the brain on the left is considerably larger, has fewer spots and less dark areas, compared to the one on the right.
According to neurologists this sizeable difference has one primary cause – the way each child was treated by their mothers.
The child with the larger and more fully developed brain was looked after by its mother – she was constantly responsive to her baby, reported The Sunday Telegraph.
But the child with the shrunken brain was the victim of severe neglect and abuse.
According to research reported by the newspaper, the brain on the right worryingly lacks some of the most fundamental areas present in the image on the left.
The consequences of these deficits are pronounced – the child on the left with the larger brain will be more intelligent and more likely to develop the social ability to empathise with others.
But in contrast, the child with the shrunken brain will be more likely to become addicted to drugs and involved in violent crimes, much more likely to be unemployed and to be dependent on state benefits.
The child is also more likely to develop mental and other serious health problems.
Professor Allan Schore, of UCLA, told The Sunday Telegraph that if a baby is not treated properly in the first two years of life, it can have a fundamental impact on development.
He pointed out that the genes for several aspects of brain function, including intelligence, cannot function.
[…]The study correlates with research released earlier this year that found that children who are given love and affection from their mothers early in life are smarter with a better ability to learn.
The study by child psychiatrists and neuroscientists at Washington University School of Medicine in St. Louis, found school-aged children whose mothers nurtured them early in life have brains with a larger hippocampus, a key structure important to learning, memory and response to stress.
The research was the first to show that changes in this critical region of children’s brain anatomy are linked to a mother’s nurturing, Neurosciencenews.com reports.
The research is published online in the Proceedings of the National Academy of Sciences Early Edition.
Lead author Joan L. Luby, MD, professor of child psychiatry, said the study reinforces how important nurturing parents are to a child’s development.
I have a very good feminist non-Christian friend who sometimes comments here. I once asked her about marriage and she said that her skills would be wasting on raising children. I explained to her my view that a mother needs to stay at home with the children, and that is more important work. I expect my future wife to read all kinds of books on child care and to give the child attention, nutrition, exercise and play so that the child will grow up to be an effective Christian. Maybe I need to be clear. I am not going to spend hundreds of thousands per child with just any woman. I need a woman who can produce influential and effective Christians who will engage in the public square. And we do not entrust that job to just anyone – we want a Michele Bachmann or a Jennifer Roback Morse. Professional women who are willing to be stay-at-home moms when it’s necessary to do that.
I expect the woman I marry (if I marry) to have a college degree, and preferably a graduate degree, and a couple of years of employment. Then she has to stay home and invest in those children through the first five years at least. After that she can stay home or work as much as she thinks is beneficial to the family goals of impacting the university, the church and the public square – as well as continuing to raise those children. It’s not a waste of her talent to make the next William Lane Craig, the next Marsha Blackburn, the next Doug Axe, or the next Edith Jones.
Probably one of the best health care policy experts writing today is Avik Roy, who writes for Forbes magazine.
Here is his latest column, which I think is useful for helping us all get better at debating health care policy. (H/T Matt from Well Spent Journey)
Excerpt:
It’s one of the most oft-repeated justifications for socialized medicine: Americans spend more money than other developed countries on health care, but don’t live as long. If we would just hop on the European health-care bandwagon, we’d live longer and healthier lives. The only problem is it’s not true.
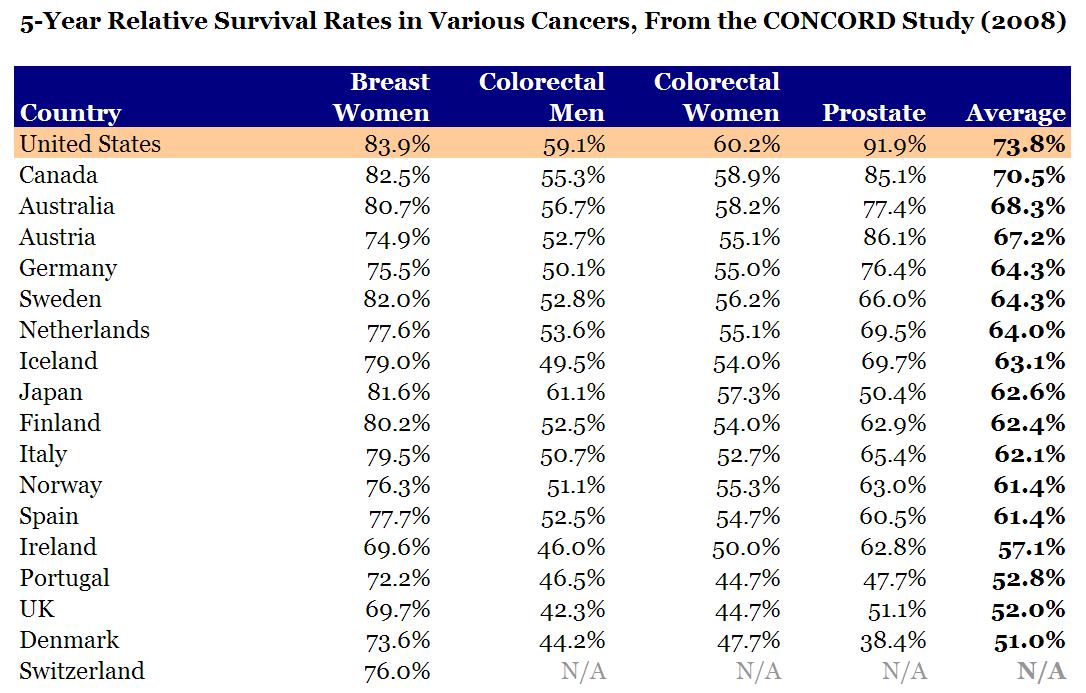
[…]If you really want to measure health outcomes, the best way to do it is at the point of medical intervention. If you have a heart attack, how long do you live in the U.S. vs. another country? If you’re diagnosed with breast cancer? In 2008, a group of investigators conducted a worldwide study of cancer survival rates, called CONCORD. They looked at 5-year survival rates for breast cancer, colon and rectal cancer, and prostate cancer. I compiled their data for the U.S., Canada, Australia, Japan, and western Europe. Guess who came out number one?
Here is the raw data:
Health care outcomes by country and type of treatment
Another point worth making is that people die for other reasons than health. For example, people die because of car accidents and violent crime. A few years back, Robert Ohsfeldt of Texas A&M and John Schneider of the University of Iowa asked the obvious question: what happens if you remove deaths from fatal injuries from the life expectancy tables? Among the 29 members of the OECD, the U.S. vaults from 19th place to…you guessed it…first. Japan, on the same adjustment, drops from first to ninth.
It’s great that the Japanese eat more sushi than we do, and that they settle their arguments more peaceably. But these things don’t have anything to do with socialized medicine.
Finally, U.S. life-expectancy statistics are skewed by the fact that the U.S. doesn’t have one health-care system, but three: Medicaid, Medicare, and private insurance. (A fourth, the Obamacare exchanges, is supposed to go into effect in 2014.) As I have noted in the past, health outcomes for those on government-sponsored insurance are worse than for those on private insurance.
To my knowledge, no one has attempted to segregate U.S. life-expectancy figures by insurance status. But based on the data we have, it’s highly likely that those on private insurance have the best life expectancy, with Medicare patients in the middle, and the uninsured and Medicaid at the bottom.
I know that my readers who like to dig deep into economics and policy will love the links at the bottom of the article:
For further reading on the topic of life expectancy, here are some recommendations. Harvard economist Greg Mankiw discusses some of the confounding factors with life expectancy statistics, citing this NBER study by June and Dave O’Neill comparing the U.S. and Canada. (Mankiw calls the misuse of U.S. life expectancy stats “schlocky.”) Chicago economist Gary Becker makes note of the CONCORD study in this blog post. In 2009, Sam Preston and Jessica Ho of the University of Pennsylvania published a lengthy analysis of life expectancy statistics, concluding that “the low longevity ranking of the United States is not likely to be a result of a poorly functioning health care system.”
The funniest thing I have found when talking to people from countries with socialized health care systems, like Canada and the UK, is that they are woefully uninformed about American health care. They literally do not know about free emergency room care, which is free for anyone regardless of insurance – including illegal aliens. They do not know about our expensive Medicaid program, which helps people who cannot afford health insurance. And our very very expensive Medicare program, which provides health care to the elderly – including prescription drugs. I get the feeling that foreign critics of American health care are getting their views from amateur documentaries produced by uneducated Hollywood propagandists, or maybe from TV shows on the Comedy Channel. They certainly are not getting their information from peer-reviewed studies by credentialed scholars from top universities, like the ones cited above.
I have literally spoken to Canadians who think that people in the USA without insurance do not get treatment and just die in the streets from stab wounds. They don’t know about the emergency room rule, or about charity care, or about Medicaid and Medicare. There is a lot of ignorance up there – wilful ignorance, in some cases. And keep in mind that the average Canadian household is paying over $11,000 a year for this substandard health care! They are paying more for less, and that’s not surprising since a large chunk of the taxes that are collected for health care go to overpaid unionized bureaucrats. Naturally, when their left-wing politicians need treatment, the first place they go is to the United States, where they pay out of pocket for the better health care. But that doesn’t stop them from denouncing American health care when they are talking to voters.
Higher infant mortality rates?
One of the other common arguments you hear from uninformed people outside the USA is the higher infant mortality rates argument.
Here’s an article by Stanford University professor Scott Atlas to explain why the argument fails.
Excerpt:
Virtually every national and international agency involved in statistical assessments of health status, health care, and economic development uses the infant-mortality rate — the number of infants per 1,000 live births who die before reaching the age of one — as a fundamental indicator. America’s high infant-mortality rate has been repeatedly put forth as evidence “proving” the substandard performance of the U.S. health-care system.
[…]n a 2008 study, Joy Lawn estimated that a full three-fourths of the world’s neonatal deaths are counted only through highly unreliable five-yearly retrospective household surveys, instead of being reported at the time by hospitals and health-care professionals, as in the United States. Moreover, the most premature babies — those with the highest likelihood of dying — are the least likely to be recorded in infant and neonatal mortality statistics in other countries. Compounding that difficulty, in other countries the underreporting is greatest for deaths that occur very soon after birth.
[…]The United States strictly adheres to the WHO definition of live birth (any infant “irrespective of the duration of the pregnancy, which . . . breathes or shows any other evidence of life . . . whether or not the umbilical cord has been cut or the placenta is attached”) and uses a strictly implemented linked birth and infant-death data set. On the contrary, many other nations, including highly developed countries in Western Europe, use far less strict definitions, all of which underreport the live births of more fragile infants who soon die. As a consequence, they falsely report more favorable neonatal- and infant-mortality rates.
[…]Neonatal deaths are mainly associated with prematurity and low birth weight. Therefore the fact that the percentage of preterm births in the U.S. is far higher than that in all other OECD countries — 65 percent higher than in Britain, and more than double the rate in Ireland, Finland, and Greece — further undermines the validity of neonatal-mortality comparisons.
You can listen to a podcast with Dr. Atlas here, from the Library of Economics web site.
A new academic study based on the Canadian census suggests that a married mom and dad matter for children. Children of same-sex coupled households do not fare as well.
There is a new and significant piece of evidence in the social science debate about gay parenting and the unique contributions that mothers and fathers make to their children’s flourishing. A study published last week in the journal Review of the Economics of the Household—analyzing data from a very large, population-based sample—reveals that the children of gay and lesbian couples are only about 65 percent as likely to have graduated from high school as the children of married, opposite-sex couples. And gender matters, too: girls are more apt to struggle than boys, with daughters of gay parents displaying dramatically low graduation rates.
Unlike US-based studies, this one evaluates a 20 percent sample of the Canadian census, where same-sex couples have had access to all taxation and government benefits since 1997 and to marriage since 2005.
While in the US Census same-sex households have to be guessed at based on the gender and number of self-reported heads-of-household, young adults in the Canadian census were asked, “Are you the child of a male or female same-sex married or common law couple?” While study author and economist Douglas Allen noted that very many children in Canada who live with a gay or lesbian parent are actually living with a single mother—a finding consonant with that detected in the 2012 New Family Structures Study—he was able to isolate and analyze hundreds of children living with a gay or lesbian couple (either married or in a “common law” relationship akin to cohabitation).
So the study is able to compare—side by side—the young-adult children of same-sex couples and opposite-sex couples, as well as children growing up in single-parent homes and other types of households. Three key findings stood out to Allen:
children of married opposite-sex families have a high graduation rate compared to the others; children of lesbian families have a very low graduation rate compared to the others; and the other four types [common law, gay, single mother, single father] are similar to each other and lie in between the married/lesbian extremes.
Employing regression models and series of control variables, Allen concludes that the substandard performance cannot be attributed to lower school attendance or the more modest education of gay or lesbian parents. Indeed, same-sex parents were characterized by higher levels of education, and their children were more likely to be enrolled in school than even those of married, opposite-sex couples. And yet their children are notably more likely to lag in finishing their own schooling.
[…]The truly unique aspect of Allen’s study, however, may be its ability to distinguish gender-specific effects of same-sex households on children. He writes:
the particular gender mix of a same-sex household has a dramatic difference in the association with child graduation. Consider the case of girls. . . . Regardless of the controls and whether or not girls are currently living in a gay or lesbian household, the odds of graduating from high school are considerably lower than any other household type. Indeed, girls living in gay households are only 15 percent as likely to graduate compared to girls from opposite sex married homes.
Thus although the children of same-sex couples fare worse overall, the disparity is unequally shared, but is instead based on the combination of the gender of child and gender of parents. Boys fare better—that is, they’re more likely to have finished high school—in gay households than in lesbian households. For girls, the opposite is true. Thus the study undermines not only claims about “no differences” but also assertions that moms and dads are interchangeable. They’re not.
With a little digging, I found the abstract of the study:
Almost all studies of same-sex parenting have concluded there is “no difference” in a range of outcome measures for children who live in a household with same-sex parents compared to children living with married opposite-sex parents. Recently, some work based on the US census has suggested otherwise, but those studies have considerable drawbacks. Here, a 20% sample of the 2006 Canada census is used to identify self-reported children living with same-sex parents, and to examine the association of household type with children’s high school graduation rates. This large random sample allows for control of parental marital status, distinguishes between gay and lesbian families, and is large enough to evaluate differences in gender between parents and children. Children living with gay and lesbian families in 2006 were about 65 % as likely to graduate compared to children living in opposite sex marriage families. Daughters of same-sex parents do considerably worse than sons.
The author of the study is a professor of economics at Simon Fraser University in British Columbia. His PhD in economics is from the University of Washington.