
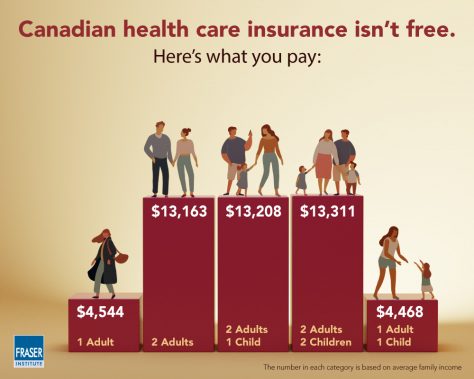
I found two interesting studies from Canada’s Angus Reid Institute describing single payer health care in Canada. I’m very interested in find out what things are like in countries that have true government-run health care. A typical Canadian family pays $13,000+ per year per household for healthcare, or about $585,000 over their working lives. What are they getting for all that money?
Here is the first Angus Reid article:
The study finds more than 2 million Canadians aged 55 and older face significant barriers when accessing the health care system in their province, such as being unable to find a family doctor or experiencing lengthy wait-times for surgery, diagnostic tests, or specialist visits.
Moreover, most Canadians in this age group have at least some difficulty getting the care they want or need in a timely manner.
The study focuses on the health care experiences of older Canadians, as well as their assessments of the quality of care they receive.
According to the article, 31% of respondents (aged 55 and older) rated access to the government’s healthcare system as “easy”. 48% had “moderate” problems with access, and 21% had “major” problems with access.
Remember: in the Canadian system, you pay your money up front in taxes, and then they decide how much healthcare you will get later – and how soon you will get it. If you worked from ages 20 to age 65, then your household will have paid 45 x $13,000 = $585,000 into the system, in order to get “moderate” problems with accessing healthcare after you’re aged 55.
And the Canadian system DOES NOT cover prescription drugs.
The second Angus Reid article explains:
This second part of the study finds one-in-six Canadians (17%) in the 55-plus age group – a figure that represents upwards of 1.8 million people – say that they or someone else in their household have taken prescription drugs in a way other than prescribed because of cost.
One-in-ten (10%) have decided to simply not fill a prescription because it was too expensive, and a similar number (9%) have decided not to renew one for the same reason. One-in-eight (12%) have taken steps to stretch their prescriptions, such as cutting pills or skipping doses.
Some 17 per cent of Canadians 55 and older have done at least one of these things, and that proportion rises among those who have greater difficulty accessing other aspects of the health care system.
In a previous blog post, I reported on how Canadians have to wait in order to see their GP doctor. If that doctor refers them to a specialist, then they have to wait to see the specialist. And if that specialist schedules surgery, then they have to wait for their surgery appointment. The delays can easily go from weeks to months and even years. The MEDIAN delay from GP referral to treatment is 19.5 weeks.
But remember – they paid into the system FIRST. The decisions about when and if they will be treated are made later, by experts in the government. This is what it means for a government monopoly to run health care. There are no free exchanges of money for service in a competitive free market. Costs are controlled by delaying and withholding treatment. And no one knows this better than elderly Canadians themselves. But by the time they realize how badly they’ve been swindled, it’s too late to get their money back out. You can’t pull your tax money out of government if you are disappointed with the service you receive. There are no refunds. There are no returns.

