
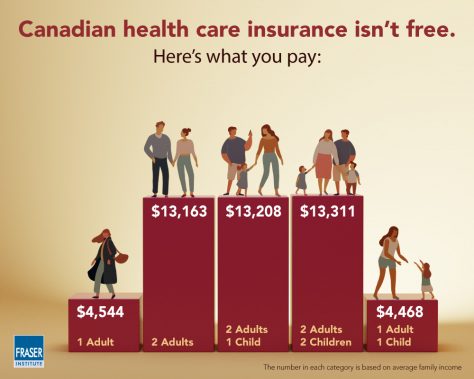
I found two interesting studies from Canada’s Angus Reid Institute describing single payer health care in Canada. I’m very interested in find out what things are like in countries that have true government-run health care. A typical Canadian family pays $13,000+ per year per household for healthcare, or about $585,000 over their working lives. What are they getting for all that money?
Here is the first Angus Reid article:
The study finds more than 2 million Canadians aged 55 and older face significant barriers when accessing the health care system in their province, such as being unable to find a family doctor or experiencing lengthy wait-times for surgery, diagnostic tests, or specialist visits.
Moreover, most Canadians in this age group have at least some difficulty getting the care they want or need in a timely manner.
The study focuses on the health care experiences of older Canadians, as well as their assessments of the quality of care they receive.
According to the article, 31% of respondents (aged 55 and older) rated access to the government’s healthcare system as “easy”. 48% had “moderate” problems with access, and 21% had “major” problems with access.
Remember: in the Canadian system, you pay your money up front in taxes, and then they decide how much healthcare you will get later – and how soon you will get it. If you worked from ages 20 to age 65, then your household will have paid 45 x $13,000 = $585,000 into the system, in order to get “moderate” problems with accessing healthcare after you’re aged 55.
And the Canadian system DOES NOT cover prescription drugs.
The second Angus Reid article explains:
This second part of the study finds one-in-six Canadians (17%) in the 55-plus age group – a figure that represents upwards of 1.8 million people – say that they or someone else in their household have taken prescription drugs in a way other than prescribed because of cost.
One-in-ten (10%) have decided to simply not fill a prescription because it was too expensive, and a similar number (9%) have decided not to renew one for the same reason. One-in-eight (12%) have taken steps to stretch their prescriptions, such as cutting pills or skipping doses.
Some 17 per cent of Canadians 55 and older have done at least one of these things, and that proportion rises among those who have greater difficulty accessing other aspects of the health care system.
In a previous blog post, I reported on how Canadians have to wait in order to see their GP doctor. If that doctor refers them to a specialist, then they have to wait to see the specialist. And if that specialist schedules surgery, then they have to wait for their surgery appointment. The delays can easily go from weeks to months and even years. The MEDIAN delay from GP referral to treatment is 19.5 weeks.
But remember – they paid into the system FIRST. The decisions about when and if they will be treated are made later, by experts in the government. This is what it means for a government monopoly to run health care. There are no free exchanges of money for service in a competitive free market. Costs are controlled by delaying and withholding treatment. And no one knows this better than elderly Canadians themselves. But by the time they realize how badly they’ve been swindled, it’s too late to get their money back out. You can’t pull your tax money out of government if you are disappointed with the service you receive. There are no refunds. There are no returns.

It’s interesting to see how much we in Canada pay for health care – so many are stuck on the “it’s free” mentality, they forget we are all still paying for it.
Also interesting is that it’s not really all that different from what the average person in the US pays. There is more of a difference in health care spending, though.
https://www.finweb.com/insurance/average-health-insurance-cost-by-country.html
“In the United States, the average health insurance cost per month is $440 for individuals and $1,100 for families, or $5,280 and $13,200 respectively per year. Much of this cost is offset by employers through an employer-sponsored group health insurance plan. The majority of the health insurance provided in the United States is through employer-sponsored plans. National health spending in the United States represents nearly 18 percent of the gross domestic product (GDP) at $2.5 trillion dollars. This number is expected to grow to $4.4 trillion by the year 2018.
…
Canada
Canada’s national health insurance program, which is similar to Medicare, accounts for 10.1 percent of the Canadian GDP. Health care spending in Canada is 8 percentage points lower than the United States. Total spending on a per capita basis is $3,895, or approximately $3,400 less than the United States. 70 percent of health spending in Canada is funded by the public sector, which is similar to the United Kingdom.”
Drawing conclusions from the information available would be a mistake, however. For many, the problem with getting a doctor is one of access, not availability. Since you specified seniors, I’ll use my mother as an example. Where she lives, health care at the clinic she went to (which was in a hospital) was mostly provided by health care practitioners (more training that nurses, but not enough to be called doctors). Her doctor came in from the city once a week. My mother has since switched to a clinic in another town. It’s a 20 minute or so drive from her place (I’m the one who drives her now, so it’s a 40 minute or so drive for me). She had no problem getting services, and the lab is across the hall. I took her to an appointment one time and, since I was there, asked if someone was available to look at a toe I’d dislocated about a week before. I actually got to see a doctor before my mother’s appointment, went across the hall to get an Xray, the results came in while I was with my mother in her appointment, so I went straight from her appointment to see the doctor that sent me for Xray. It turned out I’d broken my toe. He took a photo of the Xray so he could show it to me. When our own doctor suddenly had to move away, that left us in a lurch, but while taking my mother to another appointment for herself, I got the names of 4 doctors at that clinic that were open to new patients. We were able to get a new doctor before our old one moved away.
Some provinces have Pharmacare. We live in one of them. There is a $200 co-pay. The provincial system covers the rest. So my mother only pays $200 a year for her prescriptions. When we moved out here and set up a file at a “local” pharmacy (in another town), one of the first things they did was give us the form to fill out for Pharmacare. My daughter now works at that pharmacy. When she’s on cash, she sometimes gets customers without insurance that have to pick and choose which prescription they can afford to pay for, and it confuses me, because they should be on Pharmacare and it shouldn’t be an issue, once the co-pay is paid.
There are a lot of small differences between provinces. Some, for example, cover 1 eye test every 2 years, plus all diabetic eye tests. Others cover only the diabetic eye tests.
When it comes to things like surgery, especially for seniors, there is another problem. People like my mother. :-( She has a terrible habit of cancelling appointments or changing her mind. It took all our combined efforts to stop her from cancelling a recent hernia surgery. One of my in-laws’ mother needed hip surgery. She cancelled it at least once (I think she actually cancelled it twice) before it got done, and she died within a couple of years after (she was quite a bit younger than my mother). My brother, on the other hand, had to fight to get his hip surgery done, because they said he was “too young”. That was more than 10 years ago, and he needs to get it done again. Whether he does or not is not going to be a problem with the system, but with his waffling about it.
Waiting lists are about availability of facilities, and that’s where the biggest problem is. Usually, it’s a “first come first serve” situation, but there is triage as well; if there are cancellations, those who are more urgent cases are more likely to get called in. The other problem is access. If you are in a rural community, getting some types of care requires trips to the nearest larger city. If you’re in a fly-in community, it’s a real problem. Some people get flown to the city and have to live in whatever facility is available until their care is at a point they can be flown back home to finish treatment.
Geography plays a surprising part in whether or not someone has access to care.
LikeLike
In my province Sask. There is some drug coverage if your income is low enough. Mine is too high with my wife’s income so we luckily have my work plan that covers eighty percent of approved drugs on their list.
I don’t know what the cut off level is for our provincial drug plan since it is irrelevant to me, if I qualified for it that would only mean my work insurance plan saved money by having the gov’t pay for some of my wife’s medications.
LikeLiked by 1 person
When I lived in Alberta, one of my daughter’s co-workers was a wheelchair user on AISH. She worked part time, but had to quit her job because if she made too much money, she would loose AISH. If she lost AISH, her PT job (no benefits, of course) wasn’t enough to live on, and she would lose her prescription coverage.
My husband is on long term disability through private insurance. He makes “too much” to qualify for a lot of programs available for people with disabilities. If I got a job, it wouldn’t help because anything I made would be deducted from his disability payments. If I made too much and he no longer got payments, he would lose his insurance completely, which means no coverage on his prescriptions. We filled out the paperwork for Pharmacare, so after the deductible, the remaining amount not covered by his private insurance should be cover – but a year + later we got a letter saying they were missing tax information from me. But the form didn’t request tax information. So we’re not covered by Pharmacare.
It doesn’t seem to matter where; the systems all seem to be designed to penalize attempts to get ahead, and plenty of red tape to avoid paying out.
LikeLike
Under socialized medicine since the govt will only pay for a certain amount of a budget each year.
You have things like limits in how many people should stay overnight in the hospital. People that live alone are discharged to avoid the cost of another night in the hospital.
And only so many of each procedure is approved so they create lists that you are moved into in a que fashion.
So now instead of having it so hospitals can do more operations to make more money, they get limits from the government on how many can be done.
It is a far from perfect system and for cutting edge medical procedures it is true everyone knows if you have the money pay to get it done in the US if it is a matter of life or death if you have the means.
LikeLike
If Canadian healthcare is so great, how come every Canadian candidate running for office keeps promising to fix it? Don’t believe me, check out their campaign commercials.
LikeLike