
So, in yesterday’s post, we talked about our current budget of $4 trillion dollars, our $3 trillion of revenues, our $1 trillion annual budget deficit, and our $23 trillion in accumulated national debt. We also talked about how Elizabeth Warren’s health care plan would add $5.2 trillion to our annual budget, and how we only get about $2 trillion in revenue if we take almost everything the wealthiest taxpayers earn.
Warren likes to talk about how her plan will reduce health care costs. She thinks that government workers (think of the DMV and the post office) will be more efficient about increasing quality and reducing costs than the private sector (think of Apple and Amazon) is. Is she correct?
Let’s take a look at this article from Reason:
Warren and her defenders will likely try to shift the discussion back to total costs, but that’s just a way of repeating the dodge that has dogged her campaign for much of the year. Warren will no doubt claim that costs would go down under her plan, but there are reasons to doubt this, including an analysis from health care economist Kenneth Thorpe finding that under a Sanders-style plan, more than 70 percent of people who currently have private insurance would see costs increase, as well as an Urban Institute analysis projecting that single-payer plans would raise national health care spending by $7 trillion over a decade.
There isn’t any magic in Warren’s plan that would lover the costs to the point where the middle class would not have to pay for her spending:
Indeed, much of Warren’s plan is based on unlikely, and at times outright fantastical, assumptions about what sort of additional revenue could be raised, what health care costs could be contained, and what might be politically feasible. Among other things, she proposes raising $400 billion by passing comprehensive immigration reform, which, given the politics of immigration policy, is only a little more realistic than planning to pay off your mortgage by winning the lottery. The Washington Examiner‘s Philip Klein has published a useful roundup of Warren’s less plausible ideas; the takeaway is that even if Warren somehow managed to raise the enormous amounts of tax she proposes, it probably would still not be anywhere close to enough to finance her plan. (More on this in a future post.)
In some ways, Warren’s plan amounts to a list of technically sophisticated magic asterisks. It is as much an attempt to obscure the economic and political feasibility of passing and implementing a single-payer health care plan as a good-faith attempt to describe what it would practically require.
Yet in another way, it reveals something about both Warren and the economic reality of single-payer: Despite running a campaign based on wonky academic credentials and detail-oriented policy chops, Warren has, until now, repeatedly refused to directly answer questions about precisely how she would finance Medicare for All and whether she would foist new taxes on the middle class. Turns out she didn’t dodge the question because the answer was complex or hard to explain. She dodged it because the answer was so simple it could be expressed in a single word: yes.
So, let’s just state the obvious. We’re talking about a person who pretended to be an Indian in order to get into Harvard, and who lied about being fired from her teaching job for being pregnant. If we’re looking at her education, we don’t find any evidence that she understands health care policy, or even basic economics. If we’re looking at her work experience, there’s no evidence there that she was ever able to produce results in health care administration. There are people who have been able to reform health care in a way that reduces costs, reduces taxes, improves quality of care, and covers more people. But not Elizabeth Warren.
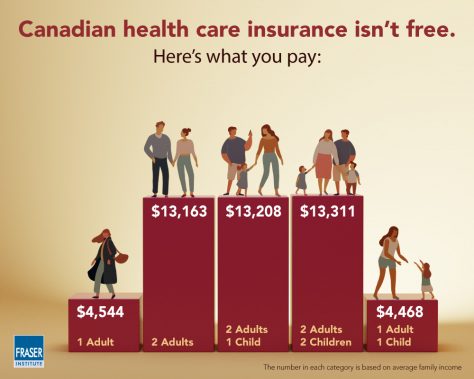
Price of healthcare per Canadian household (Source: Fraser Institute)
What about Canada?
I think it’s worth remembering how much government-run health care costs in countries that have adopted “Medicare for All” plans.
I found two interesting studies from Canada’s Angus Reid Institute describing single payer health care in Canada. I’m very interested in find out what things are like in countries that have true government-run health care. A typical Canadian family pays $13,000+ per year per household for healthcare, or about $585,000 over their working lives. What are they getting for all that money?
Here is the first Angus Reid article:
The study finds more than 2 million Canadians aged 55 and older face significant barriers when accessing the health care system in their province, such as being unable to find a family doctor or experiencing lengthy wait-times for surgery, diagnostic tests, or specialist visits.
Moreover, most Canadians in this age group have at least some difficulty getting the care they want or need in a timely manner.
The study focuses on the health care experiences of older Canadians, as well as their assessments of the quality of care they receive.
According to the article, 31% of respondents (aged 55 and older) rated access to the government’s healthcare system as “easy”. 48% had “moderate” problems with access, and 21% had “major” problems with access.
The second Angus Reid article explains:
This second part of the study finds one-in-six Canadians (17%) in the 55-plus age group – a figure that represents upwards of 1.8 million people – say that they or someone else in their household have taken prescription drugs in a way other than prescribed because of cost.
One-in-ten (10%) have decided to simply not fill a prescription because it was too expensive, and a similar number (9%) have decided not to renew one for the same reason. One-in-eight (12%) have taken steps to stretch their prescriptions, such as cutting pills or skipping doses.
Some 17 per cent of Canadians 55 and older have done at least one of these things, and that proportion rises among those who have greater difficulty accessing other aspects of the health care system.
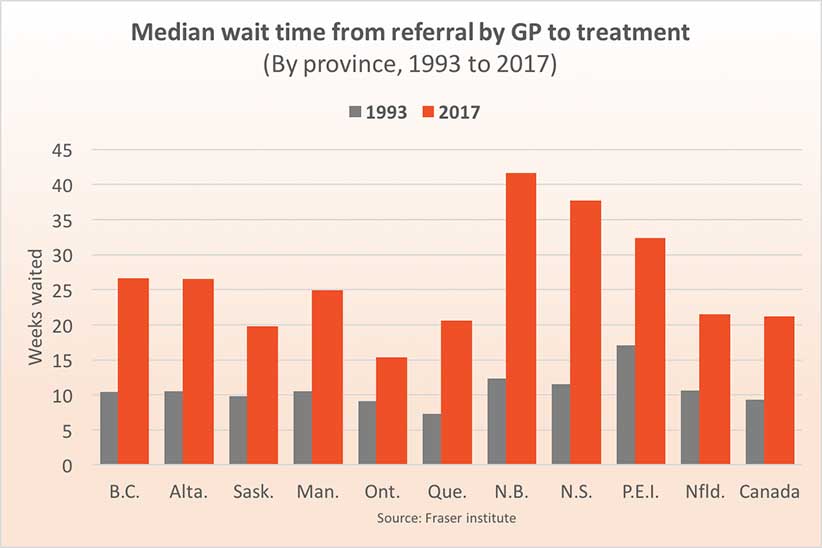
In a previous blog post, I reported on how Canadians have to wait in order to see their GP doctor. If that doctor refers them to a specialist, then they have to wait to see the specialist. And if that specialist schedules surgery, then they have to wait for their surgery appointment. The delays can easily go from weeks to months and even years. The MEDIAN delay from GP referral to treatment is 19.5 weeks.
Also, the Canadian system does NOT cover prescription drugs.
Please share this article and yesterday’s because we have an election coming up, and votes need to know the facts.
