
I post a lot of research from Canada’s Fraser Institute, but they are not the only think tank that publishes research on the efficiency and costs of single payer health care in Canada. This time, I found a report from the Heritage Foundation, where they go over quality of care, taxes, out of pocket costs, coverage, rationing, waiting lists, staff shortages, substandard equipment, and outdated drugs.
Here’s the report from the Heritage Foundation. I’ll focus on the differences.
Canadians pay slightly less in out of pocket costs:
The OECD calculates that Canadians spend 1.6 percent of GDP on out-of-pocket health spending, compared to 1.9 percent in the U.S.
[…]While these numbers are very close, they are actually getting closer. Since 1970, U.S. out-of-pocket spending as a percentage of total medical spending has been falling steadily, from 33 percent in 1970 to about 10 percent in 2017.19
Meanwhile, Canadian out-of-pocket spending has been falling much slower, so that by 2016 it totaled 15 percent of total medical spending—a higher proportion than in the U.S.20
As a result, Statistics Canada warned in early 2020 that the percentage of Canadians experiencing large out-of-pocket burdens is growing, writing that “[b]etween 1998 and 2009…the percentage of households spending more than 10% of their total after-tax income on health care rose by 56%.”
Canadians pay more in federal and state taxes:
Federal taxation excluding social security contributions, then, comes to 28 percent of GDP in Canada, compared to just 19 percent in the U.S.—meaning 51 percent more.
[…]This excess taxation is largely a result of health spending, which has bloated provincial budgets to nearly three times the taxes of U.S. states.
Provincial taxes have grown to nearly the same level as federal taxation. Meanwhile, provincial health costs have risen to fully 37 percent of provincial budgets in 2016—up from 33 percent in 1993 – —and range as high as 42 percent.
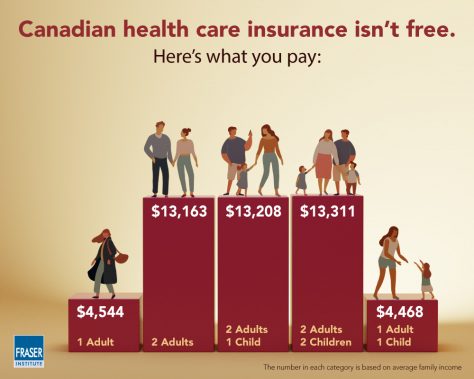
Canada’s Fraser Institute has estimated this excess tax burden from public health costs at roughly $9,000 for a household of two adults with or without children or $750 per month in additional taxes.
Canadians wait far longer for treatment than Americans:
Medical waiting times have become a national crisis in Canada, and continue to worsen. The average wait time for medically necessary treatment between referral from a general practitioner and a consultation with a specialist was 8.7 weeks in 2018, 136 percent longer than in 1993. Patients then have to wait again between seeing the specialist and the actual treatment, another 11 weeks on average, 97 percent longer than in 1993.
From referral to treatment, then, it takes an average of 19.8 weeks (see Chart 2) to be treated, in addition to the original wait to see the family doctor in the first place—this for “medically necessary” treatment, not cosmetic surgery.
In contrast, nearly 77 percent of Americans are treated within four weeks of referral, and only 6 percent of Americans report waiting more than two months to see a specialist.
As for appointments, a 2017 survey of American physicians in the 15 largest U.S. cities found that it took just 24 days on average to schedule a new-patient physician appointment, including 11 days for an orthopedic surgeon and 21 days for a cardiologist.
As a result of these long waits, by one recent estimate, at any given moment, over one million Canadians—3 percent of the entire population—are waiting for a medical treatment.
These lists can average six months, and often much longer in rural areas, which tend to suffer from doctor shortages so severe that many do not even have a family doctor. Overall, 15 percent of Canadians did not have a regular health care provider in 2017.
The shortages ripple through the system; one doctor in Ontario called in a referral to the local hospital, only to be told there was a four-and-a-half year wait to see a neurologist.
In Canada, people die or become inoperable on waiting lists:
A Montreal man was finally called for his long-delayed urgent surgery two months after he had died. One 16-year-old boy in British Columbia waited three years for an “urgent” surgery, during which time his condition deteriorated so much that he became a paraplegic.
Canadians have to travel abroad to countries with functioning health care systems in order to be treated:
These cases are, unfortunately, not isolated; a survey of specialists found that average wait times exceed what is deemed clinically “reasonable” for fully 72 percent of conditions in Canada. The situation continues to worsen every year: In 1994, the average gap between clinically reasonable delay and actual delay was only four days, and by 2018 had grown to 23 days.
[…]With one million waiting, many Canadians turn in desperation to U.S. health care—the very system some U.S. policymakers propose to transform. In 2017 alone, Canadians made 217,500 trips to other countries for health care, of which 52,500 were to the U.S., paying out of pocket to skip the waiting.
Outdated equipment, outdated drugs, staff shortages:
While the average employer-sponsored private insurance plan in Canada covers between 10,000 and 12,000 drugs, most public plans in Canada only cover 4,000. Canada has 35 percent fewer acute care beds than the U.S., and only one-fourth as many magnetic resonance imaging (MRI) units per capita—indeed, it has fewer MRI units per capita than Turkey, Chile, or Latvia.
[…]Some common treatments are simply unavailable to Canadians. For new pharmaceuticals, for example, Canada’s policy of forcing down prices so that American consumers essentially pay for Canada’s research and development has led to years-long delays for Canadian patients.
[…]Cutting corners on facilities and using outdated drugs show up in Canadian mortality rates. Thirty-day in-hospital mortality rates in Canada are 20 percent higher than in the U.S. for heart attacks, and nearly three times the U.S. level for strokes. Cancer age-standardized mortality is 10 percent higher in Canada than in the U.S.—despite far healthier lifestyles.
[…]When it comes to personnel, Canada underspends on medical staff and doctors, ranking 29th out of 33 among high-income countries for doctors per 1,000 population, accounting for a large part of those wait times. Canada has half as many specialist physicians per capita as the U.S.
[…]With such shortages and waiting lists, Canadian emergency rooms are packed. So packed that Canadians sometimes just give up and go home. Of Canadian ER visitors who are seen, 29 percent report wait times of over four hours, three times the U.S. level.
[…]Canadian seniors are 65 percent more likely to have visited the emergency room (ER) four or more times in the past year than American seniors.
Ultimately, nearly 5 percent of Canadian ER visitors end up leaving without ever being treated, giving up on a medical system that is perennially “free” but out of stock at the moment. In one study at two ERs in Alberta, 14 of the 498 walkaways were subsequently hospitalized, and one died within the week.
And keep in mind how things work in a single payer system. You pay up front through your taxes. The harder you work, the more you pay into the system. When you want treatment, you just get in line behind people who never paid one dime into the system – like all those low-skill refugees that Canada imports from Middle Eastern countries to build up the socialist voting bloc.

